Pam Long
March 29th 2023
This article was originally published on the Kim Monson website.
Pam Long explains that School mental health surveys, screenings, and assessments are third party data collection tools used to refer students to services which potentially will label students with disorders requiring psychiatric drugs and flag students for misconduct for the rest of their lives.
“The biggest drug cartels in the world get together and buy up all the media and all the politicians and force all the people in the world to stay locked up in their homes, and people can only come out if they take the cartel’s drugs and keep taking them over and over.” Woody Harrelson
School mental health surveys, screenings, and assessments are third party data collection tools used to refer students to services which potentially will label students with disorders requiring psychiatric drugs and flag students for misconduct for the rest of their lives.
Mental Health Legislation Is a Profitable Pharmaceutical Agenda
Does Colorado have a well-meaning mental health support package in the legislative process? First, consider that Democrats align with vaccine mandates, abortion, and gender transition of minors. All of these agendas put profit over people.
Mental health is very big agenda with Democrats this session: SB23-170, HB23-1130, SB23-091, HB23-1031, HB23-1200, HB23-1153, HB23-1138, HB23-1012, HB23-1007, SB23-033, HB23-1088, HB23-1013, HB23-1009, HB23-1070. These bills add mental health “assessments” in schools and refer minors to counseling without parental consent (HB-1003), expand prescriptive authority to psychologists (HB-1071), increase employment of school mental health workers (SB-004), market crisis and substance abuse services to college students (HB-1007, HB-1009), increase access for services and drugs to veterans (HB-1088), increase access to low-income individuals (SB-033, SB-091, HB-1200), and increase access to defendants accused of crimes (HB-1138, HB-1012).
Colorado is in the process of fast-tracking a dystopian mental health framework that encompasses all of society to exponentially expand prescription psychiatric drug use. HB-1153 commissions a study and report for a statewide support system (or referral system) for people with serious mental illness. HB-1130 increases drug coverage for serious mental health illness. HB-1070 reduces the post degree supervised practice time for licensure of mental health professionals. More diagnoses, more prescribers, and more drugs are on the way to students, veterans, prisoners, defendants, and low-income individuals.
If COVID was phase 1 of the pharmaceutical commandeering of state governments, then mental health legislation is phase 2 of the pharmaceutical internment of the public. Colorado Democrats now seek to further promote the pharmaceutical industry for the mental health crisis created by their pandemic policies. The vaccine mandates and blanket treatment protocols of the COVID era provide a glimpse into the one-size-fits-all type of tyrannical medical system being created. COVID lockdowns and school closures, which isolated healthy people, were not an ethical application of quarantining the sick. It is ironic that in HB23-1013 “Use of Restrictive Practices in Prisons,” Democrats acknowledge that “all less restrictive options [must] have been exhausted” before placing a prisoner in isolation with restrictions to movement, known as clinical restraint. Furthermore, the prisoner must demonstrate to be “dangerous” before subject to involuntary medications. And yet, Gov. Polis ordered every law-abiding citizen in Colorado to isolate for months from work, school, church, and most social supports. Gov. Polis also authorized employment coercion of healthcare workers in involuntary COVID vaccine mandates. Isolation and restraint require supervision to prevent harm to physical and mental health, and these are very short-term interventions due to the known harms. Democrats abandoned these principles during the pandemic, and promoted long-term social deprivation of citizens, healthcare heroes, and children—an intervention which is not even permissible with prisoners who have committed crimes. Because Democrats have irreparably broken the public trust, without remorse or apology, we must be skeptical when Democrats offer new programs for our “health and safety.”
IMatter & Healthy Kids Colorado Survey Are Not Validated Assessments for Students
Professionals in mental or behavioral health can recognize that the IMatter survey in HB1003 (for schools which opt-in to the program when it becomes law) is not an evidence-based intervention, and CDE and CDPHE are required to use evidence-based interventions. The Behavior Assessment System for Children (BASC-2) and Strengths & Difficulties Questionnaire (SDQ) are examples of validated tools.
It is unclear what the IMatter survey is measuring. Is it depression? Basic life needs? Substance abuse? The following are the first 17 questions of the “Pediatric Symptom Checklist” which offer “never,” “sometimes,” “often” responses: Fidgety, unable to sit still? Sad, unhappy? Daydream too much? Refuse to share? Do not understand people’s feelings? Feel hopeless? Have trouble concentrating? Fight with other kids? Down on self? Blame others for your troubles? Seem to be having less fun? Do not listen to rules? Act as if driven by a motor? Tease others? Worry a lot? Take things that do not belong to you? Distract easily?
First, by calling it a “symptom checklist” the authors are projecting that the respondent who answers yes to having emotions has an illness. These above 17 questions above are not symptoms of any disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM). These types of surveys are designed to create a customer for a product. In this situation, the products are counseling services, and likely a lifelong diagnosis label requiring prescriptions for psychiatric drugs.
Second, in the second section on “Life Needs” the respondent is asked to report if his/her family has basic needs: food, clothing, utilities, child care, medicine, transportation. And specifically, do you have transportation to medical appointments? Is this a tool to assess mental health, or to identify and diagnose low-income individuals? Poverty does not indicate a mental health problem. And what is the scoring system that qualifies a respondent for six “free” counseling sessions? Does one “usually” response result in a referral that becomes years of very profitable counseling sessions and copays for a prescription drug program with kickbacks to the prescriber? We would know the answers to our concerns if the assessment were the outcome of published research, with normed questions, description of test subjects, an experimental design of how the tool was field tested, and the results of using the tool.
Third, there is a three-question section on substance abuse where the respondent is asked to self-report how many days in the past year that he/she has used alcohol, marijuana, and other drugs. There are an additional six yes-or-no questions related to alcohol and drug influenced behaviors. Informed consent (right to refuse to participate) & confidentiality are ethically required before professionals ask clients to participate in any assessment or intervention. However, this tool takes a phishing approach by asking all students if they have a substance abuse problem. Substance abuse screening is reserved for people who have demonstrated at-risk behaviors and developed rapport with a trusted professional. In general, adults do not ask adults to self-incriminate (i.e. “Do you drink and drive?”), and likewise, adults should not ask minors to self-incriminate. Participation in the IMatter survey (and Healthy Kids Colorado Survey) should be viewed as the equivalent of revealing to strangers your deepest vulnerabilities in writing, and then trusting those strangers who stand to profit from your problems to assist your recovery, with the misguided hope that those same strangers will not sell your sensitive information when you request to leave their program. “Free” is the deceptive marketing strategy for programs with strings attached. And any “free” health program for minors that circumvents parental involvement by design lacks safeguards for exploitation.
Healthy Kids Colorado Survey is currently administered to middle school and high school students with 98 questions and 152 questions respectively. Parents should question how “anonymous” this survey is if students take the survey on their school assigned computers and the data is collected by third parties and shared with the state. In the demographic section students are asked about their age, grade, gender, sexual orientation (3 questions), racial and ethnic identity, mother’s education level, disability and health problems, and emotional and learning disorders. Students could be identified by this demographic data in small schools.
The survey topics include: car safety, violence related behaviors, sexual experiences (more self-incrimination with “Have you ever forced someone to have sex with you?”), bullying, self-harm, stress/suicide/sadness, tobacco use, vaping, second hand smoke, marijuana use, alcohol use, non-prescribed medications, food, concussions, home life, school, sleep, hand guns, racism, and COVID. There are no safeguards to prevent data collectors from leveraging responses for future public disclosure and revocation of rights. SB23-170 expands educators to the list of people who can petition for Extreme Risk Protection Orders to remove firearms from people with alleged mental illness without due process.
Can adults imagine their employment asking these types of highly sensitive, personal questions and collecting the data? These questions seem less likely to address health or mental health, and more likely as a priming for the social and governance expectations in companies who have adopted ESG programs as a precursor to social credit systems. These questions are a veiled way to ask questions which schools cannot ask directly without backlash such as “Do you conform to the current socially accepted values?” or “Do you blindly follow the government’s recommendations and ideology?” One can foresee future surveys will include environmental scoring such as “Does your family own an electric vehicle?”
Schools are naively collaborating with these surveys for student “health and safety,” the unchallenged cover cliché for most double-dealing government agendas. The agendas for public school students are clearly outlined in the Colorado Healthy Schools Smart Source score card for schools, which aligns with the CDC’s “Whole School, Whole Community, Whole Child Model.” Smart Source scores schools on incorporating SEL (page 17), practicing mindfulness (page 16), adopting a LGBTQ program (page 20), offering staff annual flu shots (page 24), and implementing Diversity, Inclusion, Equity programs (page 24). While government refers to these items as “health and safety” programs, most conservatives would deem these indoctrination programs. None of these programs promote education in reading, writing, or math.
CDPHE Evades COVID Suicide Epidemic Created by Lockdowns and School Closures
The Healthy Kids Colorado Survey for students and Smart Source score card for schools are both CDPHE programs. After the draconian public health policies in the pandemic, everyone should reject the notion that CDPHE values mental health. During the January 2023 CDPHE SMART hearing with the Joint Health Committee, Dr. France, CDPHE Chief Medical Officer, briefed legislators that (1) there has NOT been an increase in suicide in ten years, (2) there was a DECREASE in suicides in 2021 in 18-24 year-old people. Dr. France did not provide data to substantiate these wildly unbelievable claims. Based on national suicide reports, one should suspect that CDPHE is deliberately evading a public reckoning for its COVID guidance which resulted in significant increases in deaths of despair.
The American Academy of Pediatrics reported in a Pediatrics study (Bridge et al) using 2020 data that “There was a significant increase in overall observed versus expected youth suicides during the COVID-19 pandemic (RR = 1.04, 95% CI = 1.01–1.07), equivalent to an estimated 212 excess deaths.” Age groups with higher youth suicide deaths than before the pandemic included those aged 5 to 12 years and those aged 19 to 24 years. The mental health community predicts, as demonstrated in other disasters like Hurricane Katrina, that it will take two years to see the peak of these suicide deaths and other deaths of despair. Therefore, we can expect states to report even greater increases in suicides in 2021 and 2022.
The CDC confirms that suicides did not peak in 2020 but continued to climb in 2021. The CDC analysis found that “the average number of weekly emergency department visits for suspected suicide attempts among adolescent girls was 26% higher in the summer of 2020 and nearly 51% higher in early 2021 compared with reference periods in 2019.” A 51% increase in suicide attempts in youth is not only a public health failure; it is a catastrophe that demands accountability of all leaders who recommended long-term school closures.
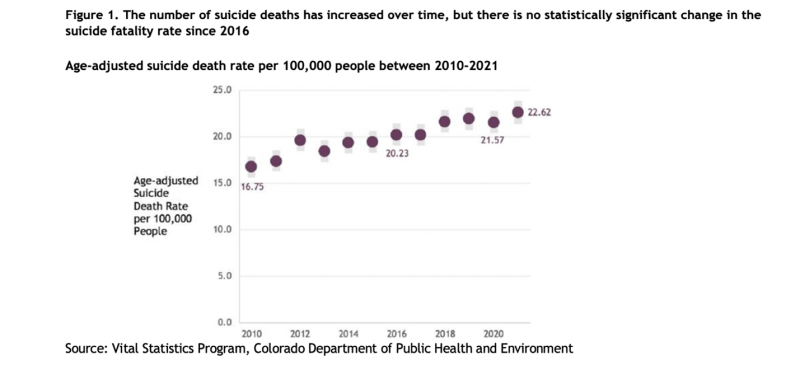
When CDPHE was forced by the Legislative Council Staff to provide the Colorado suicide data (see graph below) in response to my public comment at hearing on CDPHE’s omission of actual data, CDPHE provided data that shows (1) there has been a 35% increase in suicides in Colorado in the past decade (contrary to Dr. France briefing the legislature of no increases in ten years), and (2) CDPHE omitted the suicide rate for 2022 (the year expected to show the peak of the pandemic lockdown induced suicides) and omitted the rates for 18-24 year old people for the past ten years to include 2022 (the most vulnerable age group during the pandemic).
In rejection of CDPHE’s report that there was a decrease in youth suicides during the pandemic, the public should consider that there was a 30% increase in drug overdoses in the US, which might have been actual suicides but classified as unintentional overdoses. According to US News:
“Rajeev Ramchand, a senior behavioral scientist at the Rand Corp. and co-director of the RAND Epstein Family Veterans Policy Research Institute, says another reason why the decline in the suicide rate may not be as clear-cut as the data would suggest is if some deaths linked to another cause were actually self-inflicted.
In particular, Ramchand says he questions whether a larger portion of the more than 91,000 drug overdose deaths that occurred in 2020 – representing a more than 30% rate increase from 2019 – might have been a result of suicide. According to a CDC report on 2020 overdose deaths released in December, 91% were classified as unintentional, 4.7% as suicides, less than 1% as homicides and 4.1% as ‘of undetermined intent.’
‘Given the dramatic increase in overdose deaths coupled with the fact that medical examiners and coroner offices were so overwhelmed because of COVID, could there just have been some misclassification of suicide deaths as unintentional?’ Ramchand says. ‘The rate increase was so dramatic that I think we have to be asking that question.’”
Conclusion
Gov. Polis, CDPHE, and the Democrats in the Super Majority acted in malpractice during the pandemic and created a suicide epidemic and mental health “state of emergency” as declared by Children’s Hospital of Colorado and the American Academy of Pediatrics in 2021. These leaders who clearly lack the ability to make policy that protects children are now creating legislation to rectify the crisis they created. They cannot be trusted. Do not entrust your children to their surveys or services. Seek private care if needed outside of school and government programs so that privacy can be maintained. Parents should be livid and contacting school boards, the Colorado Department of Education, and legislators with demands that they reject these school surveys and services which circumvent parental involvement and violate student privacy. Parents can request a full disclosure of who profits from these programs in money and data, just like any other vendor of a product or service in a school. Parents can also request details on how these surveys and services are compliant with HB16-1423 Student Data Use Security.
One additional note on similar federal programs of concern, Project AWARE and The Trevor Project are two programs which educators are encouraged to direct students to regarding mental health and sexual identity. Both of these federal projects have many risks of data collection on highly sensitive personal information.
Update from HB23-1003 Fiscal Note
The bill text of HB23-1003 that passed through a House Committee proposed that schools can opt into a program offering a “mental health assessment.” The bill sponsors omitted the specific name of the mental health assessment. The bill sponsors also omitted their predicted increase in known or suspected child abuse or neglect in referrals to CPS as a result of implementing this assessment. The fiscal note provides transparency and names the assessment tool and predicts an increase in abuse reporting to CPS. Many providers stand to profit from the implementation of this bill and the subsequent referrals for either counseling or CPS involvement, which explains the 167 lobbyists registered on the Colorado Secretary of State website as working to pass HB23-1003 for mental health providers and social workers.
The HB23-1003 fiscal note also requests a staggering $17 Million a year to administer a mental health assessment: BIMAS or Behavior Intervention Monitoring Assessment System. Why was the assessment tool not specified in the bill text? My investigation reveals that BIMAS is already being tested in school districts across the state. In Boulder Valley School district, the assessment is being administered to students across the district; and in Poudre School District, the BIMAS is being administered in the School Based Health Clinic in Lincoln Middle School. BIMAS uses data from Lincoln Middle School in their “Introducing the Behavior Intervention Monitoring Assessment System (BIMAS™)” presentation to illustrate its capabilities. $17 Million a year is a profitable public-private contract. Were other assessments considered for less cost as required by the competitive bidding process?
The BIMAS is not a mental health assessment used by mental health providers in private settings. The BIMAS website clearly indicates that it is a SEL compliance monitoring tool designed for schools. SEL aims to prioritize emotional decision making over rational decision making. Democrats promote SEL because this is a necessary component to achieve Sustainable Developmental Goals, where people will be expected to forfeit their personal goals (rational thinking) for the collective good (emotional manipulation), as defined by the World Economic Forum.
This assessment will be promoted as research-based, although there is no peer review report or external validation study published in literature, with only the BIMAS authors publishing research on its validity and reliability. The notion that this is an evidence-based assessment should be challenged at CDE, which lists the BIMAS authors’ research on the CDE website without any validating research. The BIMAS will be offered to all students ages 12 and up, three times a year to measure progress on their SEL indoctrination, with a digital format collecting Personally Identifying Information (PII) by third parties contracted by CDPHE. The data will create a state reporting dashboard on the district, school, and classroom levels so that low scoring cohorts can be publicly shamed into SEL interventions to achieve a “green” rating. Due to the data mining with lifelong implications, pharmaceutical and SEL agendas, and staggering annual cost, HB23-1003 needs public backlash and opposition if the bill moves forward from the House to the Senate.